Radiology
Breast Imaging
Debra M. Ikeda, MD
Robyn L. Birdwell, MD
Kathryn F. O’Shaughnessy,
PhD
R. James Brenner, MD, JD
Edward A. Sickles, MD
Index term:
Breast neoplasms, diagnosis, 00.32,
00.30
Published online before print
10.1148/radiol.2262011634
Radiology 2003; 226:494 –503
Abbreviations:
BI-RADS ⫽ Breast Imaging Reporting
and Data System
DCIS ⫽ ductal carcinoma in situ
1
From the Department of Radiology, Stanford University Medical
Center, Rm S-068A, 300 Pasteur Dr,
Stanford, CA 94305-5105 (D.M.I.,
R.L.B.); R2Technology, Sunnyvale, Calif
(K.F.O.); Tower–St Johns Imaging
Eisenberg Keefer Breast Center, John
Wayne Cancer Institute, St John’s
Health Center, Santa Monica, Calif
(R.J.B.); and Department of Radiology,
University of California, San Francisco
(E.A.S.). From the 1999 RSNA scientific assembly. Received October 5,
2001; revision requested December
18; revision received March 14, 2002;
accepted July 24. Address correspondence to D.M.I.
Analysis of 172 Subtle
Findings on Prior Normal
Mammograms in Women with
Breast Cancer Detected at
Follow-up Screening1
PURPOSE: To retrospectively review nonspecific findings on prior screening mammograms to determine what features were most often deemed normal or benign despite
the development of breast cancer in the same location detected at follow-up screening.
MATERIALS AND METHODS: Four hundred ninety-three pairs of consecutive
mammographic findings were collected from 13 institutions, consisting of initial
normal screening findings and a subsequent finding of cancer at screening (mean
interval between examinations, 14.6 months). One designated radiologist reviewed
each pair of mammograms and determined that 286 findings were judged visible at
prior examination in locations where cancer later developed. Five blinded radiologists independently reviewed the prior findings in these 286 cases, identifying 169
mammograms (172 cancers) with findings so subtle that none or only one or two
of the five radiologists recommended screening recall. Two unblinded radiologists
reviewed the initial and subsequent findings and recorded descriptors and assessments for each finding and subjective factors influencing why, although the lesion
was perceptible, it might have been undetected or not recalled.
RESULTS: Of 172 cancers, 129 (75%) were invasive (112 T1 tumors and 17 T2
tumors or higher; median diameter, 10 mm), and 43 (25%) were ductal carcinoma
in situ (median size, 10 mm). On the prior mammograms, 80% (137 of 172) of
these cancers had subtle nonspecific findings where cancer later developed, and
most were assessed as being normal or benign in appearance.
CONCLUSION: There is a subset of cancers that display perceptible but nonspecific
mammographic findings that do not warrant recall, as judged by both a majority of
blinded radiologists and by unblinded reviewers. We believe failure to act on these
nonspecific findings prospectively does not necessarily constitute interpretation
below a reasonable standard of care.
©
Author contributions:
Guarantor of integrity of entire study,
D.M.I.; study concepts and design,
D.M.I., R.J.B.; literature research,
D.M.I., R.L.B., E.A.S., R.J.B.; clinical
studies, D.M.I., R.L.B., K.F.O.; data acquisition, D.M.I., R.L.B., K.F.O.; data
analysis/interpretation, D.M.I., R.L.B.,
E.A.S., K.F.O.; statistical analysis, D.M.I.,
K.F.O.; manuscript preparation, D.M.I.,
R.L.B., E.A.S., R.J.B.; manuscript definition
of intellectual content, all authors; manuscript editing, D.M.I., R.L.B., E.A.S., R.J.B.;
manuscript revision/review and final version approval, all authors.
©
RSNA, 2002
494
RSNA, 2002
Investigators in retrospective studies of missed breast cancers categorize previous mammograms with normal findings into mammograms in which the cancer is radiographically
occult (33%–58%) and mammograms in which a finding is perceptible but was undetected
or misinterpreted (1– 4). The latter category can be further subdivided into errors in
perception (overlooked mammographic features of cancer) and errors in analysis (misinterpretation of perceptible mammographic abnormalities).
At screening mammography, failure to act on classic or atypical findings of cancer is
usually due to errors in perception or analysis. On the other hand, failure to act on
nonspecific mammographic findings is not tantamount to an error in judgment. In
contrast to typical errors of detection or analysis, nondetection or nonaction with regard
to nonspecific findings occurs because there are no classic or atypical signs of cancer to
detect. Simply put, there are no abnormal findings to be overlooked or missed. Perceived
Radiology
but nonspecific mammographic findings
would correctly be interpreted as normal
or benign.
Few reports on missed cancers in the
radiology literature describe nonspecific
findings. The terms for nonspecific findings are often mentioned in reports of
missed cancers, but the nonspecific findings are often grouped with other categories of missed cancers (4– 6). In reviews (1–
4,6) of prior mammograms that showed
cancer at the time of screening or at time
intervals between screenings, investigators
named these findings “nonspecific signs,”
“minimal signs present,” or “unspecific appearances” or grouped nonspecific findings with “unrecognized signs.”
For purposes of the present study, we
named this last category “nonspecific findings,” defined as perceptible normal or benign mammographic findings where cancer later developed. Examples of such
nonspecific findings included focal densities or benign-appearing calcifications occurring in the location where cancer later
developed that were so nonspecific for malignancy that prospective recall from screening mammography was not warranted.
The purpose of our study was to retrospectively review these nonspecific findings on prior screening mammograms to
determine what features were most often
deemed normal or benign despite the development of breast cancer in the same
location detected at follow-up screening.
MATERIALS AND METHODS
Case Selection
Methods of mammogram collection
have been previously described (7,8).
Briefly, 13 U.S. facilities certified according to the Mammography Quality Standards Act (community-based hospitals,
health maintenance organizations, and
academic mammography centers) provided 1,083 consecutive biopsy-proven
cases of cancer detected on screening
mammograms in asymptomatic women
between 1994 and 1996 (7,8). Institutional review board approval for use of
these cases was obtained from each institution. Informed patient consent was not
required. Mean patient age was 62.3 years
(range, 40 – 86 years). The 1,083 screening mammograms that showed cancer
were evaluated by one of the 13 facility
radiologists who, with knowledge of the
biopsy-proven cancer location, marked
the cancer location on the screening
mammograms on which the cancer was
detected by using two transparent film
overlays, one for each view.
Volume 226
䡠
Number 2
TABLE 1
Interpretation and Detection Factors Recorded for 172 Subtle Findings
on Prior Screening Mammograms
No. of Factors Cited
for Possible Miss
Factor
Interpretation factors
Normal-appearing tissue
Benign-appearing calcifications
Too few calcifications
Lucent areas
Other similar calcifications
Finding too small to prompt work-up
Detection factors
Finding seen on only one view
Overlooked calcifications
Multiple findings
Finding at edge of glandular tissue
Distracting lesions
Dense breast
Finding obscured by overlying tissue or vessels
Finding at image edge
Large breast
Technical factors
92 (53)
53 (31)
40 (23)
29 (17)
21 (12)
12 (7)
37 (22)
29 (17)
22 (13)
21 (12)
19 (11)
18 (10)
13 (8)
12 (7)
6 (3)
31 (18)
Note.—Numbers in parentheses are percentages. Findings were reviewed by unblinded reviewers
(D.M.I., R.L.B.). Multiple factors recorded for each finding.
Four hundred ninety-three of the 1,083
cases with prior screening mammograms
were available for review. The mean time
between examinations was 14.6 months
(range, 9–24 months). Sixty-two of these
493 cases were excluded because of prior
breast surgery that resulted in scars or findings affected by metallic skin markers. Four
other cases were excluded because the original mammograms were needed at the facility site before the end of our study, leaving a total of 427 cases in the study cohort.
One of three board-certified radiologists, other than the facility radiologists,
reviewed the 427 cases to determine if
the cancers were visible in retrospect on
the prior mammograms. One radiologist
reviewed 242 mammograms, one radiologist reviewed 103 mammograms, and
one radiologist reviewed 82 mammograms. Each radiologist used the previously created film overlays to locate the
cancer on the mammograms. The overlay was then superimposed on the prior
mammograms with normal findings. If a
perceptible finding was deemed visible
on the prior mammogram, the radiologist marked the location of the retrospectively visible finding by using a second
set of transparent film overlays, creating
a reference location of the subsequent
cancer on the prior mammogram.
Findings were judged visible on the
prior mammograms in locations where
cancer later developed in 286 of the 427
(67%) cases. The 286 prior mammograms
were divided into four sets, each with
approximately 75 cases. Forty-five addi-
tional cases were added to each case set:
five cases in which no abnormalities
could been seen on the prior mammograms, 20 cases with small subtle cancers,
and 20 cases with normal findings (confirmed by means of at least one subsequent mammographic examination with
normal findings in the following 2 years).
To determine if the normal findings on
the prior mammograms should have
been evaluated further, four groups of
five radiologists performed a blinded review of the four case sets. The radiologists
were unaware of the study purpose and
the case mix. These 20 radiologists (10
with a primary focus in mammographic
interpretation) were all certified according to the Mammography Quality Standards Act, had practiced radiology for a
mean of 17 years (range, 3–35 years), and
had read a mean of 300 screening mammograms per month (range, 40 –1,000).
Each radiologist independently assessed
approximately 120 cases and categorized
them according to the American College
of Radiology Breast Imaging Reporting
and Data System (BI-RADS) (9). BI-RADS
categories 1 and 2 indicated normal or
benign findings, and categories 0, 4, and
5 indicated abnormal findings. The use of
category 3 (probably benign) was discouraged; however, the data showed 16
category 3 cases, which were grouped
with the category 1 and 2 cases for purposes of our study. For clarity, we will
refer to cases that the majority of five
radiologists assessed as having a BI-RADS
category of 0, 4, or 5 as abnormal, mean-
Analysis of Subtle Findings on Prior Mammograms
䡠
495
TABLE 2
Comparison of BI-RADS Categories at Unblinded Review with Number of Recalls Made by Five Blinded Radiologists
for 169 Mammograms with 172 Findings
Radiology
BI-RADS Category
No. of Radiologists to Make Recalls
Zero
One
Two
Total
No. of Cases
No. of Findings
0
1
2
4
80 (47)
51 (31)
38 (22)
82
51
39
9
10
15
31
14
5
42
27
18
0
0
1
169 (100)
172
34
50
87
1
Note.—Numbers in parentheses are percentages. Data were reviewed by unblinded reviewers (D.M.I., R.L.B.).
TABLE 3
172 Findings on Prior Screening Mammograms, Stratified for BI-RADS
Categories at Unblinded Review and Invasive Cancers versus DCIS
BI-RADS Category
0 or 4
Finding
No. of
Findings
Focal island of normal tissue
0
Benign-appearing calcifications 21 (60)
Few benign-appearing
calcifications
0
Mass
7 (20)
Density only on one view
4 (11)
Mass with calcifications
3 (9)
Other
0
Total
35
Cancer Type
BI-RADS Category
1 or 2
No. of
Findings
Cancer Type
NA
11 DCIS, 10 invasive
65 (47) 2 DCIS, 63 invasive
23 (17) 12 DCIS, 11 invasive
NA
7 Invasive
1 DCIS, 3 invasive
1 DCIS, 2 invasive
NA
24 (18)
4 (3)
5 (4)
0
16 (12)
13 DCIS, 22 invasive
137
15 DCIS, 9 invasive
4 Invasive
5 Invasive
NA
1 DCIS, 15 invasive
30 DCIS, 107 invasive
Note.—Numbers in parentheses are percentages. NA ⫽ not applicable. Data were reviewed by
unblinded reviewers (D.M.I., R.L.B.).
ing the finding required immediate action. We will refer to cases that the majority of radiologists judged as having a
BI-RADS category of 1, 2, or 3 as normal,
meaning that the findings were normal
or benign or did not require immediate
action. The blinded radiologists were provided with patient age and shown only
the prior mammograms with normal
findings (mammograms obtained 9 –24
months before the cancer was diagnosed
at screening). They were not provided
with any mammograms obtained earlier.
The blinded radiologists had 84% mean
sensitivity for cancer detection in the 20
cases with subtle findings that were
added to each case set and 81% mean
specificity for the 20 normal cases added
to each case set.
Mammograms with three or more abnormal findings at the reference location
as judged by the five blinded radiologists
were considered to have cancers that
were initially missed. The rationale is
that if a majority of radiologists in a
blinded review interpreted the findings
as needing immediate work-up, then the
finding was prospectively missed (8).
496
䡠
Radiology
䡠
February 2003
One hundred twelve mammograms were
judged as having abnormal findings according to these criteria by a majority of
the radiologists and were excluded.
Three or more of the five blinded radiologists judged the findings on the remaining 174 mammograms as normal,
benign, or requiring no immediate workup. We classified these mammograms as
having nonspecific findings by using the
rationale that if a majority of radiologists
in a blinded review interpreted the findings as normal, then the finding was very
subtle, normal, or benign in appearance.
Five of the 174 mammograms with nonspecific findings had incomplete or missing data and were excluded. The remaining 169 mammograms with 172 cancers
constituted our final study group. At the
time of the initial study, all mammograms were digitized with an LS85 digitizer (Lumisys, Sunnyvale, Calif) at
50-m resolution and printed with an
Imation HQ969 laser printer (Imation
Enterprises, St Paul, Minn) at 12 bits per
pixel and 100-m resolution. These digitized images were then printed on film
for subsequent case review.
Unblinded Radiologist Case Review
The purpose of the unblinded review
was to have radiologists who specialized
in breast imaging and who knew the reference location of the subsequent cancer
assess the findings independently, to retrospectively reconfirm BI-RADS categories, to categorize the appearance of each
finding, and to determine the reasons
why the findings were so nonspecific as
to merit prospective assessments of BIRADS categories 1, 2, and 3 by a majority
of the blinded radiologists. Two radiologists (D.M.I., R.L.B.) who specialized in
breast imaging jointly reviewed the 169
mammograms in an unblinded review to
categorize the findings and to assess possible reasons for nondetection and nonaction at initial assessment. To ensure
that the digital copies were of sufficient
quality for analysis, 20 original mammograms selected to include both masses
(n ⫽ 12) and calcifications (n ⫽ 8) were
recalled from the facility sites and compared side by side with the copies on
dedicated mammography alternators.
The original mammogram and the copies
were rated by the two radiologists for image quality with a numerical rating of 1–5
(1 ⫽ unable to read, 3 ⫽ acceptable, and
5 ⫽ good) and a narrative description of
mass or calcification visibility. The average quality ratings for the original images
(4.5) and for the copies (4.4) were similar.
The narrative descriptions indicated that
the copy quality did not compromise
mass or calcification detection, which
further supports the acceptability of using image copies for our study.
To assess the mammographic characteristics of the visible findings, the 169
prior mammogram copies with normal
findings, subsequent follow-up mammograms on which the cancers were detected, and the clear reference overlays
were reviewed with a two-tiered dedicated motorized mammography alternator with bright lights and magnifying
Ikeda et al
Radiology
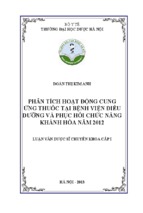
Figure 1. Focal island of normal tissue rated as BI-RADS category 1 at unblinded review and cited for recall by only one of five radiologists at
blinded review. (a) Craniocaudal and (b) mediolateral oblique views in a 64-year-old woman show a focal region of normal-appearing glandular
tissue (arrow) perceived on the mediolateral oblique view only. Note that the finding has lucent areas within it. Thirteen months later,
(c) craniocaudal and (d) mediolateral oblique mammograms show a 1.0-cm suspicious mass (arrows) in the same location. Biopsy results indicated
grade II invasive ductal carcinoma.
lenses available for use. The four-view
prior mammogram with normal findings
and the reference overlay were displayed
on the top row, and the mammogram
showing the cancer 9 –24 months later
with the reference overlay were displayed
on the bottom row. At the time of case
review, although the location of the subsequent cancer was available on the followup mammograms, no patient information,
examination dates, or pathologic data were
available to the reviewers.
The perceptible finding identified with
the reference overlay on the prior mammogram was analyzed according to finding type, diameter, location, and depth
Volume 226
䡠
Number 2
within the breast. Breast density was also
recorded. Each finding was categorized
by using the BI-RADS lexicon for masses
and calcifications and BI-RADS categories
0 –5, excluding BI-RADS category 3 (9). As
we endeavored to fully describe all findings, we added several non–BI-RADS
terms to describe the normal and benign
findings not addressed in the lexicon.
Terms for nonspecific findings included
focal islands of normal-appearing tissue,
benign-appearing calcifications, few benign-appearing calcifications, and densities. Otherwise, findings were characterized by using the BI-RADS lexicon when
possible. The term that best described the
major character of the perceived finding
was chosen as the finding type.
To explain possible reasons why the
findings were originally interpreted as
normal, we (D.M.I., R.L.B.) recorded features that might have led to dismissal of
the finding, including an appearance of
focal normal tissue, benign-appearing
calcifications, too few calcifications to
prompt patient recall, lucent lines within
the finding that simulated intermixed fat
or crossed Cooper ligaments, other similar calcifications in the breast, or findings
too small to prompt work-up. We also
recorded features that may have led to
nonperception or nondetection of the
Analysis of Subtle Findings on Prior Mammograms
䡠
497
Radiology
Figure 2. Benign-appearing area, too small to prompt recall, rated as BI-RADS category 2 at unblinded review and recalled by no radiologists at
blinded review. (a) Craniocaudal and (b) mediolateral oblique mammograms in a 64-year-old woman show a 3-mm round dense area (arrows) in
the upper inner quadrant of the right breast. Twelve months later, (c) craniocaudal and (d) mediolateral oblique mammograms show a 7-mm mass
(arrows) in the same location. Biopsy results indicated grade III invasive ductal carcinoma.
finding, including findings seen on only
one view, subtle clusters of calcifications,
multiple findings in the breast, a single
benign but prominent and distracting lesion, a finding located at the edge of the
glandular tissue or at the edge of the image, dense breast tissue, focal overlying
breast tissue or blood vessels that might
obscure the finding, and a very large
breast in which small lesions might be
missed. Multiple factors were recorded
for each lesion, if appropriate.
498
䡠
Radiology
䡠
February 2003
We reviewed the pathology reports for
each cancer that was subsequently detected on the follow-up screening mammogram and compared each subtle finding on the prior mammogram with the
subsequent cancer type and grade.
Statistical Analysis
A 2 test for concordance (CHITEST
Function; Microsoft Excel, Redmond,
Wash) was prepared to determine if more
invasive carcinomas developed in recalled versus nonrecalled cases.
RESULTS
The 169 patients had an average age of
62.3 years, with 16 (9%) patients aged
40 – 49 years, 50 (30%) aged 50 –59 years,
58 (34%) aged 60 – 69 years, 40 (24%)
aged 70 –79 years, and five (3%) aged 80
years or older. In 9% (16 of 169) of cases,
Ikeda et al
Radiology
the breast tissue was assessed as fatty,
46% (78 of 169) had scattered fibroglandular densities, 32% (54 of 169) had heterogeneously dense tissue, and 12% (21
of 169) had extremely dense tissue.
One hundred seventy-two cancers
were detected at follow-up screening
mammography in the 169 patients. The
average time between the prior screening
examination with normal findings and
the cancer diagnosis assigned at follow-up screening was 14.6 months
(range, 9 –24 months). Forty-three (25%)
of the 172 cancers were ductal carcinoma
in situ (DCIS), and the remaining 129
(75%) were invasive cancers at the time
of diagnosis. The median lesion size of
DCIS was 10 mm (range, 2–75 mm).
Twenty-four of 43 (56%) DCIS sizes were
obtained from the pathology report, and
the rest were obtained from the mammographic measurement of abnormal calcifications. The median lesion size of invasive cancers was 10 mm (range, 1–55
mm). One hundred nineteen of 129
(92%) invasive cancer sizes were obtained
from the pathology report, and the rest
were obtained from measurement of the
abnormal finding on mammograms. Of
invasive cancers, 112 were T1 tumors,
and 17 were T2 or higher. Of 104 women
with invasive cancer and known axillary
node status, 22 (21%) had lymph nodes
positive for metastatic disease.
Table 1 summarizes features that might
have contributed to nondetection of findings as judged at unblinded review.
Table 2 summarizes the number of
cases and findings recalled by the five
blinded radiologists compared with those
recalled by the unblinded experts. All five
blinded radiologists rated nearly half (80
cases, 47%) of the 169 cases as normal at
review. Fifty-one of the 169 cases (30%)
were rated as normal by four of the five
blinded radiologists, and 38 of 169 (22%)
were rated as normal by three of the five
blinded radiologists (Table 2).
At unblinded review, with knowledge
of the subsequent cancer location, the
two unblinded radiologists would have
recalled 35 (20%) of the 172 findings,
rating them as BI-RADS category 0 or 4
(Table 2). Twenty-six of these 35 cases
(74%) would have required immediate
action as judged by one or two of the five
blinded radiologists. At unblinded review, the remaining 137 (80%) of the 172
findings were considered normal or benign, even in retrospect, by the two unblinded radiologists, and all of these findings were judged as BI-RADS category 1
and 2 with knowledge of the subsequent
cancer location. None of the five blinded
Volume 226
䡠
Number 2
Figure 3. Benign-appearing calcifications that could be easily overlooked, rated as BI-RADS
category 2 at unblinded review and recalled by no radiologists at blinded review. Magnification
of (a) craniocaudal and (b) mediolateral oblique mammograms in a 69-year-old woman show
three benign-appearing calcifications (arrows). Fourteen months later, (c) craniocaudal and
(d) mediolateral oblique mammograms show a 4-mm cluster of pleomorphic calcifications
(arrows) in the same location. Biopsy results indicated DCIS with an intermediate grade.
radiologists would have recalled 73 (53%)
of these 137 findings.
Table 3 summarizes the types of findings considered normal on prior screening mammograms, stratified into cases
interpreted as normal in retrospect at unblinded repeat review (137 findings) and
recall cases at unblinded repeat review
(35 findings). The two categories of unblinded normal and recall cases are further subdivided into invasive cancers and
DCIS found subsequently for each type of
finding.
Findings at unblinded repeat review
showed a marked difference in the 137
normal findings versus the 35 recall findings. Of the 137 normal findings confirmed at unblinded review, the most
common finding was a focal island of
normal tissue (65 findings, 47% of normal findings) (Figs 1, 2), followed by few
benign-appearing calcifications (24 findings, 18%) (Fig 3), a benign-appearing
calcification cluster (23 findings, 17%),
densities seen on only one view (five
findings, 4%), masses (four findings, 3%)
(Fig 4), and other findings (16 findings,
12%; primarily asymmetric densities,
subtle possible distortion, and dilated
duct). None of these findings had suspicious features for cancer; specifically,
there were no pleomorphic calcifications,
suspicious mass margins or shapes, or
other findings suspicious for cancer.
At unblinded repeat review, 35 cases
needed recall in retrospect. In contradistinction to the 137 normal cases, the 35
recall cases contained no focal islands of
normal tissue or few benign-appearing
calcifications. Most (21 findings, 60%) of
the unblinded recall findings were composed of benign-appearing calcifications
Analysis of Subtle Findings on Prior Mammograms
䡠
499
Radiology
Figure 4. Benign-appearing mass rated as BI-RADS category 2 at unblinded review that was recalled by no radiologists at blinded review. (a) Craniocaudal and (b) mediolateral oblique mammograms in a 64-year-old woman show several benign-appearing equal-density masses, with one of the masses
(arrows) in the area of interest. Subsequent screening (c) craniocaudal and (d) mediolateral mammograms obtained 14 months later show a 1-cm mass
(arrows) in the left breast, which was pathologically proven to be grade I invasive ductal carcinoma with cribriform and micropapillary DCIS.
that also contained some pleomorphic
forms (Fig 5), seven masses (20%) that
had suspicious margins or shapes (Fig 6),
and four densities (11%) that were seen
on only one view but had suspicious features that warranted recall on the basis of
only that projection.
To determine if invasive cancers developed more frequently in the unblinded
recall group versus the normal group, we
analyzed cancer types developing at the
site of unblinded BI-RADS category 0 and
4 findings compared with those developing at the site of BI-RADS category 1 and
2 findings (Tables 3, 4). Invasive carcino500
䡠
Radiology
䡠
February 2003
mas subsequently developed at the site of
63% (22 of 35 cancers) of the unblinded
recall findings and also at the site of 78%
(107 of 137 cancers) of the normal findings. Results of the 2 test were not significant (P ⫽ .06) for this comparison.
Table 4 summarizes the results of the
unblinded repeat review regarding interpretation and detection factors that may
have led to nonrecall. Multiple interpretation and detection factors were recorded for each finding (mean, 2.7 factors). These results have been further
stratified for invasive cancers versus DCIS
and for unblinded recall cases versus nor-
mal cases. Multiple interpretation and
detection factors were recorded for each
finding (mean, 2.7 factors). There was a
difference between factors related to normal findings on the prior screening
mammograms of the 129 invasive cancers compared with those of the 43 DCIS
cases (Table 4). Most of the 129 invasive
cancers (88 of 129, 68%) looked like normal tissue on the prior mammogram;
others were seen on only one view (28 of
129, 22%) or had lucent lines that simulated fat running through the finding (26
of 129, 20%). In contradistinction, the
findings in the 43 DCIS cases were domIkeda et al
Radiology
inated by microcalcifications—specifically, benign-appearing calcifications (30
of 43, 70%), too few calcifications to
prompt recall (23 of 43, 53%), or small
clusters that may have been overlooked
(16 of 43, 37%).
DISCUSSION
False-negative findings on screening
mammograms contribute to increased
breast cancer mortality rates (1,4). Our
population differs from that in many
prior investigations of false-negative
mammographic findings because we focused on nonspecific findings that are
perceptible and detectable but that are so
normal or benign in appearance that
most would not be recalled, even in retrospect. Indeed, three, four, or all five
blinded radiologists interpreted any
given case in this study population as
normal or benign or not needing immediate recall. Results of our unblinded repeat review confirmed a subset of cases
with findings that were still judged as
normal or benign by radiologists who
specialize in breast imaging and who
knew the location and appearance of the
subsequent cancer. Thus, our data set differs substantially from that in most studies that focus on detection errors or misinterpretation of abnormal findings.
The results of our study demonstrate
that there are subsets of perceptible but
nonspecific findings on prior mammograms that should not be considered
observer or interpretation errors. These
nonspecific findings are composed mostly
of densities that are indistinguishable
from randomly distributed islands of fibroglandular tissue or scattered groups of
tiny calcifications that most commonly
represent fibrocystic change. Even though
137 of such findings were not recalled by
a majority of five blinded radiologists
and were judged as normal or benign at
unblinded repeat review, 107 invasive
cancers (78%) and 30 cases of DCIS (22%)
developed at the same location as the
subtle finding and were detected on follow-up screening mammograms 9 –24
months later.
Few investigators describe nonspecific
normal or benign findings on prior
screening mammograms to serve as a
comparison for our study. Unrecognized
mammographic findings are often composed of both nonspecific findings and
atypical but misinterpreted features of
breast cancer. The minimal signs reported by van Dijck et al (10) comprised
vague densities in 15 of 32 (47%) cases,
Volume 226
䡠
Number 2
Figure 5. (a) Craniocaudal mammogram in a 62-year-old woman with clustered microcalcifications
(arrow) in the right breast, which were rated as BI-RADS category 0 at unblinded review and were
recalled by only one of five radiologists at blinded review. (b) Screening craniocaudal mammogram
obtained 13 months later shows a 1.2-cm DCIS, seen as pleomorphic calcifications (arrow).
densities in five (16%), microcalcifications in eight (25%), densities and microcalcifications in one (3%), and architectural distortion in three (9%). Similarly,
our 137 nonspecific findings confirmed
at unblinded review mostly comprised
noncalcified findings, such as focal islands
of fibroglandular tissue, masses, and densities (74 of 137, 54%), while fewer findings
comprised calcifications (47 of 137, 34%).
In a previous study, Ikeda et al (4) found 21
(22%) slightly abnormal findings that
showed nonspecific signs in 96 interval
cancers, including six nonspecific densities, four asymmetries, four benign-appearing calcification clusters, and four benign
masses. Similar to those in the present
study, the nonspecific signs of cancer in
the study of Ikeda et al (4) were dominated
by benign-appearing soft-tissue findings.
In two studies in which recall from
mammographic screening would not be
recommended, results were similar to
ours. Wolverton and Sickles (5) prospectively evaluated 583 “doubtful mammographic findings” on screening mammograms in 382 women, in which all
findings but one (low-grade DCIS) were
normal at a mean follow-up interval of
30 months. Of note, most of their doubtful mammographic findings were composed of benign-appearing calcifications
(48%), while the rest were noncalcified
nodules (22%), vague densities (18%),
asymmetries (7%), or a combination of
findings (2%) that were interpreted as benign. The authors concluded that almost
all of these prospectively marked benign
findings were benign and inconsequential. Maes et al (6) reviewed nonspecific
minimal signs (vague densities with an
unsharp border, less than six clustered
indefinable microcalcifications, and subtle architectural distortions) in a large
population in the Netherlands to determine the frequency of recall and the effect these findings had on the screening
program. Their nonspecific minimal signs
were found in 53 (11%) of 500 women
with normal or benign mammographic
findings. The authors concluded that, on
the basis of breast cancer prevalence and
incidence in the Netherlands, the additional risk of such women developing
breast cancer is about 0.5% and that regular mammographic screening, rather than
recall, is a reasonable option. The results of
these two studies show that nonspecific
findings occur frequently in mammographic screening programs and that most
do not represent cancer.
One limitation of our study was the
lack of even older mammograms for comparison with the prior screening mammograms with normal findings. It is conceivable that comparison with these older
mammograms might have shown that the
nonspecific normal findings on our prior
mammograms may have been either developing or new, warranting recall. We
simply cannot tell or predict which of
these cases could have been in this category. On the other hand, if the finding had
been shown on an initial screening mammogram, as was simulated during the
blinded review by the five radiologists,
most radiologists would have interpreted
the finding as normal. This shows that our
case set contained findings that were very
subtle or appeared benign or normal.
Analysis of Subtle Findings on Prior Mammograms
䡠
501
Radiology
Figure 6. (a) Mediolateral oblique (left) and craniocaudal (right) mammograms in
a 75-year-old woman with a subtle spiculated mass (arrows) in the right breast. The
mass was rated as BI-RADS category 0 at unblinded review and was recalled by only
one of five radiologists at blinded review. (b) Mediolateral oblique (left) and craniocaudal (right) mammograms obtained 12 months later show a larger spiculated
mass (arrows). Note that the mass is slightly more anterior on the mediolateral
oblique view than on the mediolateral oblique view in a because of differences in
obliquity. Pathologic findings showed a 1.5-cm invasive lobular carcinoma.
Another limitation of the current study
is the second retrospective unblinded review that was necessary to characterize
each subtle finding in this case set and to
reconfirm BI-RADS categories. Unblinded
retrospective reviews inherently lead to unintentional bias and may have led to the
higher number of abnormal readings not
evident in the initial blinded review by the
five radiologists. Harvey et al (11) showed
that nonpalpable breast cancers are often
detected in retrospect on prior mammograms but that retrospective reviewers de502
䡠
Radiology
䡠
February 2003
scribed the findings as suspicious more often than did blinded reviewers, a difference
that was statistically significant. In their
retrospective study, blinded reviewers were
shown 73 prior mammograms with normal findings in patients who subsequently
developed cancer, 30 (41%) of whom had
mammographic evidence of cancer. The
blinded reviewers interpreted these remaining 43 (59%) mammograms as normal, but retrospective reviewers found evidence of cancer (mostly asymmetric
densities) on 25 mammograms (34%).
Thus, it is not surprising that our unblinded review resulted in 35 suspicious
findings in retrospect, likely because of the
increased tendency of retrospective reviewers to detect abnormalities on mammographic review.
A possible criticism of our study is the
initial grouping of BI-RADS category 3
cases with the BI-RADS category 1 and 2
cases. The 16 BI-RADS category 3 readings
were a small percentage of all blinded readings, consisting of 1.8% (16 of 845) of all
the readings in the 169 cases by the five
radiologists. While this practice was discouraged in the initial blinded review,
some radiologists still rated a few cases as
BI-RADS category 3. We do not endorse
this practice for clinical use, and in our
practices, we do not allow final categorization of cases into BI-RADS category 3 without a recall from screening and a diagnostic work-up. For purposes of the present
study, we grouped the 16 BI-RADS category
3 cases with BI-RADS category 1 and 2 cases
by reasoning that these categories constituted findings that required no immediate
action. Thus, one of the purposes of the
second unblinded review was to have the
two radiologists reconfirm overall BI-RADS
categories. In this way, we could search for
those findings that constituted BI-RADS
category 1 and 2 cases at repeat review with
the understanding that there are unintentional study biases introduced (addressed
in the previous paragraph).
Interpretive error, involving either detection or diagnosis of breast cancer, is the
most common reason that radiologists are
sued for malpractice (11). At issue in such
cases of alleged negligence is whether the
abnormality identified on a prior mammogram should have been recalled or diagnosed as a suspicious finding by a reasonable and prudent radiologist practicing
under similar circumstances (12). The essential element of such an analysis concerns foreseeable outcome; namely, is it
reasonably foreseeable that the mammographic finding in question represents evidence of malignancy (13)? Conversely, is it
reasonably foreseeable that the mammographic finding in question does not represent evidence of malignancy? The law
requires neither a warranty of certainty nor
accuracy, but it does require a reasonable
approach (12,14,15).
The results of our study provide a basis
for indicating which types of lesions may
in fact represent cancer but which lack reasonable foreseeable outcome in a medicolegal context to necessarily prompt further
evaluation because they are so nonspecific
and are more likely to represent benign
findings and normal variants. Expert witIkeda et al
Radiology
TABLE 4
Interpretation and Detection Factors for 172 Findings on Prior Screening Mammograms, Stratified for BI-RADS Categories
at Unblinded Review and Invasive Cancers versus DCIS
BI-RADS Category
0 or 4
Factor
Interpretation factors
Normal-appearing tissue
Benign-appearing calcifications
Too few calcifications
Lucent areas
Other similar calcifications
Finding too small to prompt work-up
Detection factors
Seen on only one view
Overlooked calcifications
Multiple findings
Finding at edge of glandular tissue
Distracting lesions
Dense breast
Finding obscured by overlying tissue or vessels
Finding at image edge
Large breast
Technical factors
No. of
Factors
No. of Findings
(n ⫽ 35)
92 (53)
53 (31)
40 (23)
29 (17)
21 (12)
12 (7)
7 (20)
10 (29)
7 (20)
9 (26)
2 (6)
4 (11)
1
6
3
2
2
1
DCIS,
DCIS,
DCIS,
DCIS,
DCIS
DCIS,
37 (22)
29 (17)
22 (13)
21 (12)
19 (11)
18 (10)
13 (8)
12 (7)
6 (3)
31 (18)
5 (14)
16 (46)
6 (17)
9 (26)
5 (14)
3 (9)
6 (17)
6 (17)
5 (14)
7 (20)
2
9
2
2
2
3
2
3
2
4
BI-RADS Category
1 or 2
No. of Findings
(n ⫽ 137)
Cancer Type
3 invasive
85 (62)
43 (31)
33 (24)
20 (15)
19 (14)
8 (6)
3 DCIS, 82 invasive
24 DCIS, 19 invasive
20 DCIS, 13 invasive
1 DCIS, 19 invasive
7 DCIS, 12 invasive
4 DCIS, 4 invasive
DCIS, 3 invasive
DCIS, 7 invasive
DCIS, 4 invasive
DCIS, 7 invasive
DCIS, 3 invasive
Invasive
DCIS, 4 invasive
DCIS, 3 invasive
DCIS, 3 invasive
DCIS, 3 invasive
32 (23)
13 (9)
16 (12)
12 (9)
14 (10)
15 (11)
7 (5)
6 (4)
1 (1)
24 (18)
7 DCIS, 25 invasive
7 DCIS, 6 invasive
1 DCIS, 15 invasive
12 Invasive
3 DCIS, 11 invasive
3 DCIS, 12 invasive
7 Invasive
3 DCIS, 3 invasive
1 Invasive
10 DCIS, 14 invasive
Cancer Type
6
4
4
7
invasive
invasive
invasive
invasive
Note.—Numbers in parentheses are percentages. Multiple factors were recorded for each finding. Findings were reviewed by unblinded reviewers
(D.M.I., R.L.B.).
nesses reviewing cases of alleged negligence
must distinguish between nonspecific findings that do not require recall and more important abnormalities that merit prompt additional imaging evaluation. To be fair and
reasonable, expert reviews should be conducted in a manner that minimizes interpretation bias by blinding the reviewer to the
location, mammographic features, and timing of subsequent cancer (similar to the
blinded reviews of the four groups of five
radiologists described in our study). In the
setting of a medicolegal consultation, this
can be achieved most effectively by viewing
mammograms in the temporal sequence in
which they were obtained and by limiting
the reviewer’s access to supporting clinical
information to that known by the interpreting radiologist at the time of examination.
If prior findings are sufficiently specific
and suspicious to prompt recall, failure to
do so may fall below a recognized standard of care. However, when mammographic findings are present in the area
that later develops more specific features
of malignancy, and those earlier findings
are nonspecific or subthreshold, the results of our study support the notion that
failure to recall the patient does not necessarily fall below the standard of care.
Thus, the mere presence of a prior finding in a patient who was not recalled at the
time of screening does not constitute medical negligence or unreasonable interpretation, which is the basis for liability in an
allegation of malpractice. None of our paVolume 226
䡠
Number 2
tients were recalled prospectively, given
the limitations of the study design, and
137 of the cases were judged as having a
BI-RADS category of 1 or 2 at unblinded
repeat review, supporting the contention
that at least some of these findings should
not necessarily be recalled. These 137 perceptible but nonspecific findings did not
warrant recall as judged by a majority of a
group of five blinded radiologists and by
two unblinded reviewers, and failure to recall these cases does not constitute diagnostic error.
In summary, the results of our study
show that there is a class of nonspecific
findings that are perceptible on prior
screening mammograms that do not warrant recall, and despite their presence in a
location where cancer would later develop, we believe failure to identify these
findings prospectively does not necessarily constitute interpretation below a reasonable standard of care.
5.
6.
7.
8.
9.
10.
11.
References
1.
Frisell J, Eklund G, Hellstrom L, Somell A.
Analysis of interval breast carcinomas in a
randomized screening trial in Stockholm.
Breast Cancer Res Treat 1987; 9:219 –225.
2. Holland R, Mravunac M, Hendriks JH, Bekker
BV. So-called interval cancers of the breast.
Pathologic and radiologic analysis of sixtyfour cases. Cancer 1982; 49:2527–2533.
3. Martin JE, Moskowitz M, Milbrath JR. Breast
cancer missed by mammography. AJR Am J
Roentgenol 1979; 132:737–739.
4. Ikeda DM, Andersson I, Wattsgard C, Janzon L,
Linell F. Interval carcinomas in the Malmo
Mammographic Screening Trial: radiographic
12.
13.
14.
15.
appearance and prognostic considerations. AJR
Am J Roentgenol 1992; 159:287–294.
Wolverton DE, Sickles EA. Clinical outcome
of doubtful mammographic findings. AJR
Am J Roentgenol 1996; 167:1041–1045.
Maes RM, Dronkers DJ, Hendriks JH, Thijssen
MA, Nab HW. Do non-specific minimal signs
in a biennial mammographic breast cancer
screening programme need further diagnostic assessment? Br J Radiol 1997; 70:34 –38.
Warren Burhenne LJ, Wood SA, D’Orsi CJ, et
al. Potential contribution of computer-aided
detection to the sensitivity of screening mammography. Radiology 2000; 215:554 –562.
Birdwell RL, Ikeda DM, O’Shaughnessy KF,
Sickles EA. Mammographic characteristics of
115 missed cancers later detected with
screening mammography and the potential
utility of computer-aided detection. Radiology 2001; 219:192–202.
American College of Radiology. Breast imaging
reporting and data system (BI-RADS). 3rd ed. Reston, Va: American College of Radiology, 1998.
van Dijck JA, Verbeek AL, Hendriks JH, Holland R. The current detectability of breast
cancer in a mammographic screening program: a review of the previous mammograms
of interval and screen-detected cancers. Cancer 1993; 72:1933–1938.
Harvey JA, Fajardo LL, Innis CA. Previous
mammograms in patients with impalpable
breast carcinoma: retrospective vs. blinded
interpretation. AJR Am J Roentgenol 1993;
161:1167–1172.
Physicians Insurers Association of America.
Breast cancer study. Rockville, Md: Physicians Insurers Association of America, 1995.
Skeffington v Bradley, 366 Mich 552, 115
NW2d, 3030 (Mich 1962).
Brenner RJ. Medical legal aspects of breast
cancer evaluation and treatment. In: Harris
JR, Lippman ME, Hellman S, eds. Diseases of
the breast. Philadelphia, Pa: LippincottRaven, 1996; 125–133.
Todd v Eitel Hospital, 237 NW2d 357, 79
ALR 3d 907 (Minn 1975).
Analysis of Subtle Findings on Prior Mammograms
䡠
503
- Xem thêm -